



Çocuk Kalp Hastalıkları ve Cerrahisi (Pediatric Heart Diseases and Cardiac Surgery)
Çocuk Kalp Cerrahisi Platformu (Platform for Pediatric Heart Surgery)
Pediatrik Kalp Hastalıkları ve Cerrahisi
Pediatric Heart Diseases and Cardiac Surgery
Aort koarktasyonu
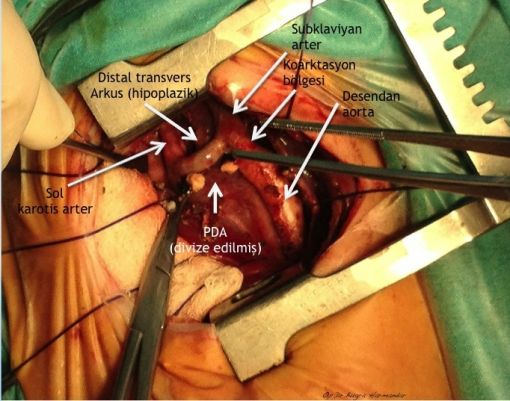
Aort Koarktasyonu

Aort koarktasyonu
Koarktasyon tipleri
Aort koarktasyonu tamiri
Arkus aorta hipoplazisi + aort koarktasyonlu uygun vakalarda arkus aorta rekonstrüksiyonunu off-pump (kardiyopulmoner bypass kullanılmaksızın) gerçekleştiriyoruz. Kardiyopulmoner bypass kullanılmaksızın gerçekleştirilen bu işlem sayesinde hem ameliyat riski hem de hastaların yoğun bakımda kalış süreleri ciddi oranda azalıyor.









Patofizyoloji
Aortic coarctation is a congenital narrowing of the aorta, usually distal to the origin of the left subclavian artery, opposite the area of the ductus arteriosus at the aortic isthmus. Varying degrees of aortic arch hypoplasia may coexist. In the newborn, the presence of a patent ductus arteriosus will often allow adequate lower body perfusion. Presentation may vary from acute decompensation at the time of ductal closure in the infant, to upper extremity hypertension in the older child or adult. Identification of elevated pressures in the upper versus lower extremities is useful in making the diagnosis of aortic coarctation.
Cerrahi teknik
Repair of aortic coarctation is usually performed via a left thoracotomy without cardiopulmonary bypass. There are a number of techniques available to repair the coarctation, each with its own advantages and disadvantages.
1. Left subclavian patch angioplasty.
In this technique, the left subclavian artery is isolated and divided distally. The vessel is then opened longitudinally with extension of the incision on to the aorta. The subclavian artery flap is then folded down over the area of aortic narrowing and sutured into place. Subclavian patch angioplasty has a number of advantages over other techniques. This technique is relatively simple, it allows for the use of the patient's own tissue, it has a low recurrence rate, and it provides excellent relief of the obstruction. A relative disadvantage is that the subclavian artery is sacrificed in the subclavian flap angioplasty technique. Transient decreased perfusion to the left arm has been observed in older patients who have undergone repair using this technique, but limb threatening ischemia is rare. Associated aortic arch hypoplasia is not addressed with this technique.
2. Resection with end-to-end anastomosis.
With resection and end-to-end anastomosis, the aorta is isolated and the aortic isthmus and ductal tissue are resected. The distal aortic arch is incised along its inferior side, the lower aorta is incised along its lateral side, and the two are sewn together. The advantages of end-to-end technique are that the subclavian artery is not sacrificed, and complete relief of obstruction is easily obtained. The end-to-end aortoplasty technique is the procedure of choice for many surgeons today, especially in patients beyond the newborn period. A variation of the classic end-to-end repair is the Extended end-to-end technique. This technique is similar to the classic end-to-end repair of coarctation of the aorta discussed above, but differs in that the aortic arch is incised more proximally along its lesser curvature, and the lower aorta is incised further along its posterior-lateral aspect. The two ends are then brought together and anastomosed. The advantage of this variation is that relief of aortic arch hypoplasia is possible since the aortic arch is more widely opened, and therefore, obstruction is more readily relieved. Extended end-to-end repair may prove to be the operation of choice since aortic arch hypoplasia is now thought to be more prevalent than previously recognized.

3. Subclavian translocation.
With the subclavian artery translocation technique, the subclavian artery is isolated and transected at its origin. A longitudinal incision is made along the medial aspect of the subclavian artery and also along the anterior aspect of the aorta. The two segments are then anastomosed as depicted in the diagram. The advantages of this repair technique are similar to the advantages in the subclavian flap angioplasty technique, but since the subclavian artery is reimplanted, the vessel is not sacrificed. A disadvantage of this technique is that the aorta and subclavian artery must be extensively mobilized and tension on the suture line may make recurrence more likely.

4. Synthetic patch angioplasty (not shown)
With synthetic patch angioplasty, the aorta is isolated, the site of coarctation is opened with proximal and distal extension of the incisions, and a patch of synthetic material or homograft is sutured into place. This method of repair has the advantage of being technically simple, relatively quick, offers a low rate of recurrence, and provides excellent relief of the obstruction. The use of prosthetic material has been associated with late aneurysm formation. It is thought that newer materials may decrease the potential for this complication.
Postoperative Considerations
The postoperative course following repair of coarctation of the aorta is usually uncomplicated. Invasive monitors commonly utilized include arterial and central venous catheters. Systemic hypertension is often encountered in the postoperative period, and usually responds to nitroprusside or intravenous beta blockers. Uncontrolled rebound hypertension may result in ileus or, more rarely, bowel necrosis. Later in the hospital stay, intravenous anti-hypertensive medications are switched to orally administered beta blockers and/or afterload reducing agent such as captopril or enalapril. As with patent ductus arteriosus surgery, the recurrent laryngeal branch of the vagus nerve is near the operative site and occasional hoarseness is encountered following surgery. This is usually transient and resolves spontaneously. Paraplegia is a rare postoperative complication, and is related to spinal cord ischemia during repair. Postoperative bleeding requiring reoperation is rare. Length of hospital stay required following repair of coarctation of the aorta averages four to seven days.



Yorumlar - Yorum Yaz

- "Doğumsal Kalp Hastalıklarında Palyatif Prosedürler" isimli kitabımız açık kaynak olarak Üniversitemiz yayınevi tarafından yayınlandı.

- Prof.Dr.Buğra HARMANDAR, Muğla SK Üniversitesi Tıp Fakültesi Fakülte Kurulu Profesör Temsilciliğine 3 yıl süre ile seçildi.

- Çocuk Kalp Cerrahisi Platformu artık Muğla'da...

- Çift Arkus Aorta (Double Aortic Arch) nedeniyle ameliyatını yaptığımız 11 hastalık serimizin sonuçları yayınlandı.

- Modifiye Mee Şantı nedir? (Modified Mee Shunt)
- İFLAS EDEN FONTAN DOLAŞIMI “GÜNCEL CERRAHİ VE MEDİKAL TEDAVİ SEÇENEKLERİ” başlıklı makalemiz İstanbul Tıp Fakültesi Dergisi'nde yayınlandı...
- Hastalarımızdan gelen sorular ve cevapları yayınlandı.
- Çift Arkus Aorta (Double Aortic Arch) ameliyatını nasıl yapıyoruz?
- Pulmoner Hipertansiyon - Kimi opere edelim ? Kimi opere etmeyelim ?
- Ebstein Anomalisi - Cerrahi Tedavi Seçenekleri
- ASD (Atrial septal defekt) operasyonlarını minimal invazif (estetik) gerçekleştiriyoruz.