



Çocuk Kalp Hastalıkları ve Cerrahisi (Pediatric Heart Diseases and Cardiac Surgery)
Çocuk Kalp Cerrahisi Platformu (Platform for Pediatric Heart Surgery)
Pediatrik Kalp Hastalıkları ve Cerrahisi
Pediatric Heart Diseases and Cardiac Surgery
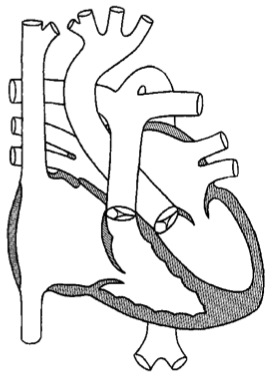
Interrupted aortik ark
Kesintili Aortik Arkus (IAA)
Doç.Dr.Buğra Harmandar
Interrupted Aortic Arch
Pathophysiology
Interrupted aortic arch is characterized by interruption of the aortic arch distal to the left subclavian artery (Type A), proximal to the left subclavian artery (Type B), or between the innominate artery and the left common carotid artery (Type C). Blood supply to arterial distributions proximal to the interruption is provided by the ascending aorta. Blood supply to arterial distributions distal to the interruption is provided by a patent ductus arteriosus. Arterial oxygen saturation proximal to the interruption is normal, while the arterial oxygen saturation distal to the interruption is lower than normal. Closure of the patent ductus arteriosus in patients with interrupted aortic arch results in lower body hypoperfusion and acidosis. Infusion of prostaglandin E1 to maintain ductal patency is an important component of resuscitation and preoperative stabilization. Ventricular septal defect is a frequent association, especially with Types B and C. Surgical correction of this anomaly is performed during the neonatal period.
Surgical Technique
Type A interrupted aortic arch without VSD or with a small VSD is usually repaired much like coarctation of the aorta with end-to-end anastomosis (see Coarctation of the Aorta). As the site of interruption moves more proximally, the patient is more likely to have a nonrestrictive VSD and a one stage repair of the aortic arch and intracardiac anomalies is performed. Repair of type B and C interrupted aortic arch requires cardiopulmonary bypass, with deep hypothermia and circulatory arrest. Since there is interruption of the aorta, a unique cardiopulmonary bypass technique is utilized. The arterial limb of the cardiopulmonary bypass circuit is divided into two arms. Perfusion of the proximal aorta is accomplished with one arm, and perfusion of the distal aorta is accomplished with the other arm via cannulation of the patent ductus arteriosus. Once total body hypothermia has been attained, cardiopulmonary bypass is discontinued and the cannulae are removed. Direct anastomosis of the upper aortic and lower aortic segments is usually possible. With recannulation of the aorta in the traditional way, cardiopulmonary bypass is resumed. Associated defects such as ventricular septal defect and atrial septal defect are now repaired. Transesophageal echocardiography, proximal and distal aortic pressure measurements and oxygen saturation comparison are utilized to confirm adequacy of repair. Delayed sternal closure is sometimes required following this repair.
Postoperative Considerations
The postoperative course following repair of type B or C interrupted aortic arch with ventricular septal defect can be variable. This operation represents a major undertaking for a neonate. Preoperative pulmonary overcirculation or recent resuscitation from ductal closure could result in hemodynamic instability in the postoperative period. Invasive monitors utilized following repair include arterial, central venous and left atrial catheters. An oximetric catheter placed in the pulmonary artery is utilized to monitor pulmonary artery pressure and cardiac output. Vasoactive infusions required for hemodynamic management might include dopamine or dobutamine, epinephrine, milrinone, nitroprusside or phenoxybenzamine, and norepinephrine. Sedation with intravenous infusions of fentanyl and a neuromuscular blocking agent is often required to reduce pulmonary artery hypertensive episodes. Inhaled nitric oxide has proven useful in the management of pulmonary artery hypertension. Postoperative bleeding is a rare complication, but may occur since the surgical repair involves suture lines exposed to systemic level pressure. Atrioventricular conduction disturbance is a potential complication since the surgical procedure involves working near the atrioventricular conduction tissue. Temporary pacing capability should be readily available. Postoperative arterial oxygen saturation and intracardiac pressures should be normal. Length of hospital stay following repair of interrupted aortic arch is variable, but two weeks or more is average.

Yorumlar - Yorum Yaz

- "Doğumsal Kalp Hastalıklarında Palyatif Prosedürler" isimli kitabımız açık kaynak olarak Üniversitemiz yayınevi tarafından yayınlandı.

- Prof.Dr.Buğra HARMANDAR, Muğla SK Üniversitesi Tıp Fakültesi Fakülte Kurulu Profesör Temsilciliğine 3 yıl süre ile seçildi.

- Çocuk Kalp Cerrahisi Platformu artık Muğla'da...

- Çift Arkus Aorta (Double Aortic Arch) nedeniyle ameliyatını yaptığımız 11 hastalık serimizin sonuçları yayınlandı.

- Modifiye Mee Şantı nedir? (Modified Mee Shunt)
- İFLAS EDEN FONTAN DOLAŞIMI “GÜNCEL CERRAHİ VE MEDİKAL TEDAVİ SEÇENEKLERİ” başlıklı makalemiz İstanbul Tıp Fakültesi Dergisi'nde yayınlandı...
- Hastalarımızdan gelen sorular ve cevapları yayınlandı.
- Çift Arkus Aorta (Double Aortic Arch) ameliyatını nasıl yapıyoruz?
- Pulmoner Hipertansiyon - Kimi opere edelim ? Kimi opere etmeyelim ?
- Ebstein Anomalisi - Cerrahi Tedavi Seçenekleri
- ASD (Atrial septal defekt) operasyonlarını minimal invazif (estetik) gerçekleştiriyoruz.